≤1 pt: low probability
2-3 pts: intermediate probability
≥4 pts: high probability
| Criterion | Points |
ECG findings:
| |
>QTc: | |
>= 480 ms | 3 |
460-470 ms | 2 |
450 ms (men) | 2 |
torsades de pointes | 2 |
Twave alternans | 1 |
notched T wave in 3 leads | 1 |
Low heart rate for age (resting HR below 2nd percentile for age | 0.5 |
Clinical history:
| |
Syncope | |
With stress | 2 |
Without stress | 1 |
Congenital deafness | 0.5 |
Family history
| |
Family members with definite LQTS | 1 |
Unexplained SCD at age 30 yrs among immediate family members | 0.5 |
Notes::
| |
| |
| LQTS type | Chromosome | Gene | Protein | Ion current | Triggers | Notes |
|---|---|---|---|---|---|---|
1 |
11p15.5 | KCNQ1 | KvLQT1 (Kv7.1) | IKs | exercise (swimming), emotion |
|
2 |
7q35-36 | KCNH2 | HERG (Kv11.1) | IKr | rest, emotion, exercise (acousting, post-partum) |
|
3 |
3p24-21 | SCN5A | Nav15 | INa | rest, sleep, emotion |
|
4 |
4q24-27 | ANK2 | Ankyrin-B | INa, INa-Ca, INa-K | exercise | |
5 |
21q22 | KCNE1 | MinK | IKs | exercise, emotion |
|
6 |
21q22 | KCNE2 | MRP1 | IKr | rest, exercise | |
7 |
17q23 | KCNJ2 | Kir2.1 | IK1 | rest, exercise |
|
8 |
12p13.3 | CACNA1C | CAV1.2 | KCa | exercise, emotion |
|
9 |
3p25.3 | CAV3 | Caveolin-3 | INa | non-exertional, sleep | |
10 |
11q23.3 | SCN4B | NaVß4 | INa | exercise, post-partum |
|
N/A |
10p15.5 | CACNB2b | CAVß2b | ICa |
|
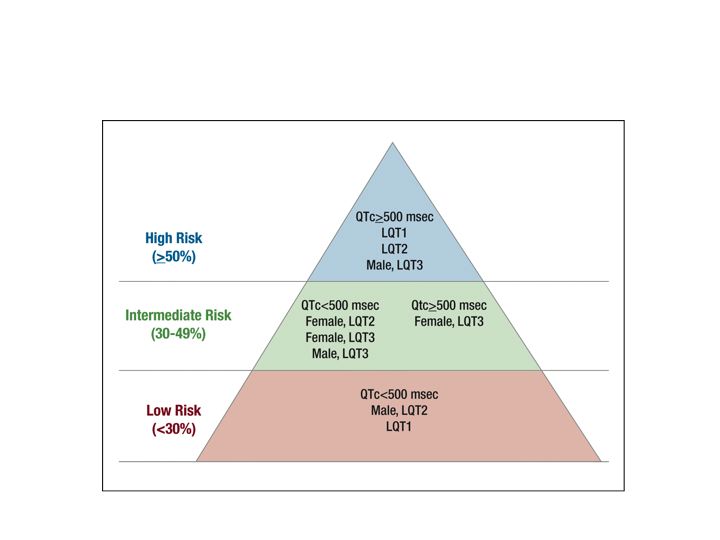
LQTS Risk Pyramid